Australian Asthma Handbook
The National Guidelines for Health Professionals
Australian Asthma Handbook
The National Guidelines for Health Professionals
Cite
Read first
Table
| Feature | Consider: |
| Symptoms present from birth | Cystic fibrosis Structural abnormality Bronchopulmonary dysplasia Primary ciliary dyskinesia |
| Abnormal voice | Acute viral laryngitis Vocal cord nodules Structural abnormalities Inducible laryngeal obstruction |
| Sudden breathlessness at rest | Panic attacks |
| Cough | |
| Acute onset | Inhaled foreign body |
| Dry cough occurring during daytime only | Somatic cough (previously called ‘habit’ cough) |
| Persistent productive cough | Bronchiectasis Cystic fibrosis Primary ciliary dyskinesia Protracted bacterial bronchitis |
| Persistent cough | Post-viral cough Allergic rhinitis Primary ciliary dyskinesia Pertussis |
| 🚩Cough with haemoptysis | Infection Inhaled foreign body Congestive heart disease Vascular abnormality Bronchial mass Cystic fibrosis |
| Upper respiratory tract | |
| Chronic production of sputum | Protracted bacterial bronchitis |
| Nasal polyps | Cystic fibrosis |
| Chest sounds | |
| 🚩 Unilateral wheeze | Inhaled foreign body |
| No variation in wheeze | Structural abnormality |
| Inspiratory wheeze | Inducible laryngeal obstruction |
| Sudden wheeze at rest | Panic attacks |
| Exercise-induced wheeze that stops immediately when exertion ceases | Inducible laryngeal obstruction Anxiety |
| Stridor | Croup Inducible laryngeal obstruction |
| Localised crepitation | Pneumonia |
| Cardiac murmur | Congenital heart disease |
| Skin and integument | |
| Finger clubbing | Cystic fibrosis Primary ciliary dyskinesia Bronchiectasis Immunodeficiency |
| Systemic signs | |
| Weight loss/lack of weight gain | Immunodeficiency |
| Fevers | Chronic infection |
| Growth failure | Cystic fibrosis Immunodeficiency |
| Recurrent or atypical infections | Immunodeficiency |
Additional information
These findings require further investigation or specialist referral. Flag symbol 🚩 indicates urgent referral needed.
Table
| Asthma more likely | Asthma less likely |
More than one of the typical asthma signs/symptoms: wheeze, difficulty breathing, feeling of tightness, in the chest, cough Signs/symptoms frequent Signs/symptoms worse at night and in the early morning Signs/symptoms triggered by exercise, exposure to pets, cold air, damp air, emotions, laughing Signs/symptoms occur when child doesn’t have a cold History of allergies (e.g. allergic rhinitis, atopic dermatitis, food allergies) Family history of allergies Family history of asthma Widespread wheeze heard on auscultation Signs/symptoms respond to treatment trial of reliever, with or without a preventer Lung function measured by spirometry increases in response to rapid-acting bronchodilator Lung function measured by spirometry increases in response to a treatment trial with inhaled corticosteroid (where indicated) | Symptoms only occur when child has a cold, but never between colds* Isolated cough in the absence of wheeze or difficulty breathing History of moist cough Exercise-induced dyspnoea with noisy inspiration Chest pain Dizziness, light-headedness or peripheral tingling Repeatedly normal physical examination of chest when symptomatic Focal wheeze Normal spirometry when symptomatic (children old enough to perform spirometry) No response to a trial of asthma treatment with adequate dose and correct inhaler technique Clinical features that suggest an alternative diagnosis |
Additional information
* In preschool children, wheezing that only occurs during viral respiratory infections may not be due to asthma, but this finding does not rule out asthma. Viral respiratory infection is the most common trigger for severe acute asthma exacerbations in children of all ages.
Ask about:
In children, wheezing is more specific to asthma than cough or breathing difficulty.[Gaillard 2021, de Jong 2020]
History features that suggest an alternative diagnosis, including red flags, are listed in Table:
The probability of asthma is higher if signs and symptoms are frequent, triggered by common asthma triggers, and there is a family history of allergies or asthma.
de Jong CCM, Pedersen ESL, Mozun R, et al. Diagnosis of asthma in children: findings from the Swiss Paediatric Airway Cohort. Eur Respir J 2020; 56: 2000132.
Gaillard EA, Kuehni CE, Turner S, et al. European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5-16 years. Eur Respir J 2021; 58: 2004173.
Royal Children’s Hospital Melbourne’s What is asthma? video for parents explaining how to identify wheeze and other signs
Include the following components:
Recommendation type: Consensus recommendation
Royal Children’s Hospital Melbourne’s What is asthma? video for parents explaining how to identify wheeze and other signs.
Physical examination findings that suggest an alternative diagnosis, including red flags, are listed in Table: Signs and symptoms that suggest an alternative diagnosis in children. [[In Key tables & figures panel]]
Usually no abnormalities are detected on physical examination of a child with asthma.
Objective confirmation of wheeze is useful. If wheeze is not detectable during the consultation, ask parents to record an episode (video or audio).
The chest may be silent in severe acute asthma.
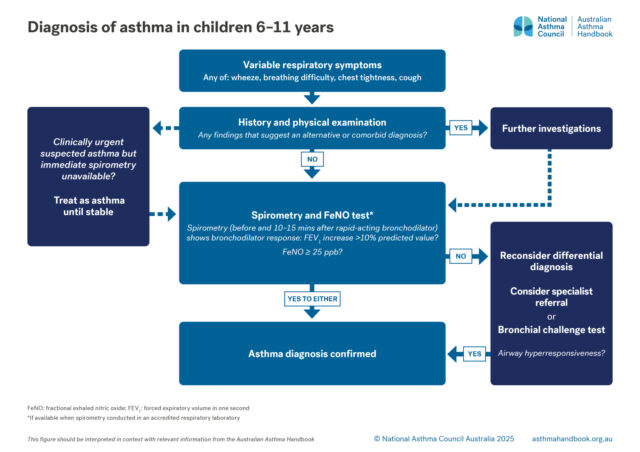
If spirometry is not available within the practice, refer to an accredited respiratory function laboratory and request spirometry and FeNO in same session. Do not delay treatment, if indicated.
Bronchodilator responsiveness (whether respiratory airflow limitation is ‘reversible’) should be tested by measuring FEV1 before, and 10–15 minutes after, administration of a rapid-acting bronchodilator (e.g. salbutamol), with at least three spirometry manoeuvres each time.
Recommendation type: Consensus recommendation
Most children aged 6–11 years can perform spirometry to acceptable quality standards in primary care.[Lo 2020]
Clinical diagnosis based solely on history leads to significant overdiagnosis of asthma.[Yang 2017]
A positive bronchodilator responsiveness test confirms the diagnosis of asthma in a child with a history of signs and symptoms suggestive of asthma.[GINA 2025]
Normal spirometry when the child is asymptomatic does not exclude asthma. Repeated spirometry (with or without other tests) may be needed.
FEV1 <80% of the child’s predicted value (according to sex, age and weight) indicates abnormal lung function.
Reduced ratio of forced expiratory volume in one second (FEV1) to forced vital capacity (FVC) indicates expiratory airflow limitation. Normal spirometry when the child is asymptomatic does not exclude asthma.
Bronchodilator responsiveness is tested by measuring FEV1 before and 10–15 minutes after administration of a rapid-acting bronchodilator (e.g. salbutamol), with at least three spirometry manoeuvres each time. The test is positive if the absolute increase in FEV1 is greater than 10% of the predicted FEV1 value for the individual.
Blake T, Chang A, Chatfield MD et al. Global Lung Function Initiative (GLI)-2012 ‘other/mixed’ spirometry reference equation provides the best overall fit for Australian Aboriginal and/or Torres Strait Islander children and young adults. Respirology 2020; 25: 281-288.
Brazzale D, Hall G, Swanney MP. Reference values for spirometry and their use in test interpretation: a position statement from the Australian and New Zealand Society of Respiratory Science. Respirology 2016; 21: 1201-9.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org.
Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med 1999; 159: 179-187.
NAC. The spirometry handbook for primary care. Melbourne; National Asthma Council Australia: March 2023. Available from: nationalasthma.org.au/resources.
Lo DK, Beardsmore CS, Roland D, et al. Lung function and asthma control in school-age children managed in UK primary care: a cohort study. Thorax 2020; 75: 101-107.
Quanjer PH, Stanojevic S, Cole TJ et al. Multi-ethnic reference values for spirometry for the 3-95 year age range: the global lung function 2012 equations. Eur Respir J 2012; 40: 1324-1343.
Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J 2022; 60: 2101499.
Yang CL, Simons E, Foty RG, et al. Misdiagnosis of asthma in schoolchildren. Pediatr Pulmonol 2017; 52: 293-302.
TSANZ’s list of accredited respiratory function laboratories
National Asthma Council Australia’s spirometry training and tools
National Asthma Council Australia’s Spirometry handbook for primary care
Definitions of positive bronchodilator response in children differ between guidelines [NAC 2023, GINA 2025, Stanojevic 2022] and between spirometer software packages:
Recommended reference values for spirometers:[NAC 2023] Global Lung Initiative (GLI) 2012 reference dataset,[Quanjer 2012, Brazzale 2016] which includes values for age ranges 3–95 years and for relevant ethnic groups.
When performing spirometry for Aboriginal and/or Torres Strait Islander people, the GLI-2012 category ‘other/mixed’ should be selected.[Blake 2020] The use of reference values obtained from the third US National Health and Nutrition Examination Survey (NHANES III)[Hankinson 1999] is no longer recommended.[NAC 2023]
More information: Lung function tests
Recommendation type: Recommendation adapted from ERS 2021
FeNO ≥25 ppb supports the diagnosis of asthma in a child with spirometry indicating expiratory airflow limitation and signs and symptoms strongly suggesting asthma. In children and adolescents aged 5–18 years, a FeNO level > 24 ppb has a reported sensitivity of 0.50 and specificity of 0.91 for the diagnosis of asthma.[BTS-NICE-SIGN 2024]
Normal FeNO level does not rule out asthma.
British Thoracic Society, National Institute for Health and Care Excellence, Scottish Intercollegiate Network. Asthma: diagnosis, monitoring and chronic asthma management (BTS, NICE, SIGN). NICE guideline [NG245]: National Institute for Health and Care Excellence [UK]; 2024. Available from: https://www.nice.org.uk/guidance/ng245.
[ERS 2021] Gaillard EA, Kuehni CE, Turner S, et al. European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5-16 years. Eur Respir J 2021; 58: 2004173.
Högman M, Bowerman C, Chavez L, et al; Global Lung Function Initiative FENO Task Force. ERS technical standard: Global Lung Function Initiative reference values for exhaled nitric oxide fraction (FENO50 ). Eur Respir J 2024; 63: 2300370.
The FeNO test is available in accredited respiratory function laboratories. Age restrictions differ between laboratories.
Normal reference ranges for FeNO vary between measuring devices and testing protocols.[Högman 2024]
FeNO is elevated in the presence of active type-2 inflammation of the airway associated with asthma. It is also elevated in some other inflammatory conditions (e.g. allergic rhinitis).
FeNO is suppressed by obesity, and by treatment with ICS and systemic corticosteroids.
The FeNO test is more useful for ruling in a diagnosis of asthma than ruling it out. A normal FeNO level does not rule out asthma.
More information on tests for airway inflammation
Recommendation type: Consensus recommendation
National Asthma Council Australia’s Spirometry handbook for primary care
Reduced FEV1/FVC ratio (< lower limit of normal for population matching child’s demographic group) indicates expiratory airflow limitation.
Expiratory airflow limitation is variable if it fluctuates more than in the healthy population (e.g. as demonstrated by a positive bronchodilator responsiveness test).
Spirometry is frequently normal in a child with asthma if conducted at a time when symptoms are absent. If FEV1 is at or near predicted value, no obstructive pattern is detected, and the bronchodilator responsiveness test is negative, spirometry should be repeated on a different occasion.
FeNO ≥25 ppb supports the diagnosis of asthma in a child with spirometry indicating expiratory airflow limitation and signs and symptoms strongly suggesting asthma.[BTS-NICE-SIGN 2024]
Recommendation type: Consensus recommendation
Peak expiratory flow is less reliable than spirometry in adults and adolescents. In children younger than 12 years it cannot reliably be used to confirm an asthma diagnosis because peak expiratory flow measurements are high variable.
Recommendation type: Consensus recommendation
Suitable specialists for referral include paediatricians, paediatric respiratory physicians, and allergists.
The specialist may arrange a bronchial challenge test. Airway hyperresponsiveness demonstrated by a positive bronchial challenge test confirms the diagnosis of asthma in a child with signs and symptoms suggesting asthma.
More information on bronchial provocation tests
Confirm that more than one episode has occurred.
Confirm that the sound reported by the child or parents is actually wheeze – ask parents to video/audio record the wheeze to verify.
Recommendation type: Consensus recommendation
Parents may not be able to recognise the difference between wheezing, stridor, snoring or normal breathing.[Fernandes 2011] Careful questioning or recordings may be necessary to correctly identify respiratory signs.
Fernandes RM, Robalo B, Calado C, et al. The multiple meanings of "wheezing": a questionnaire survey in Portuguese for parents and health professionals. BMC Pediatr 2011; 11: 112.
Royal Children’s Hospital Melbourne’s What is asthma? video for parents explaining how to identify wheeze and other signs
Recommendation type: Consensus recommendation
Asthma is among the most common causes of chronic cough in children with no abnormality detected on physical examination, chest radiography or spirometry.[Marchant 2024] Asthma may cause episodic cough that is associated with expiratory wheeze and/or exertional dyspnoea.[Marchant 2024]
In children, cough due to asthma typically resolves within one month of treatment with ICS.[Marchant 2024] ICS treatment not indicated unless there are specific features to suggest asthma.[Marchant 2024]
Chronic cough in the absence of other symptoms/signs is rarely due to asthma.[Marchant 2024] Other causes of chronic cough in children include respiratory tract infections, airway anomaly, aspiration, rhinitis/rhinosinusitis and somatic cough syndrome.[Marchant 2024, Kantar 2022]
Kantar A, Marchant JM, Song WJ, et al. History taking as a diagnostic tool in children with chronic cough. Front Pediatr 2022;10: 850912.
Marchant JM, Chang AB, Kennedy E, et al. Cough in Children and Adults: Diagnosis, Assessment and Management (CICADA). Summary of an updated position statement on chronic cough in Australia. Med J Aust 2024; 220: 35-45.
Routinely ask about coughing (frequency and quality), even if parents or carers do not mention cough.
Recommendation type: Consensus recommendation
Chronic cough in Aboriginal and Torres Strait Islander children may be under-reported because it is so common that is considered normal by parents and caregivers.[Morey 2013]
Historically, chronic suppurative lung disease has been highly prevalent among Aboriginal and Torres Strait Islander children in remote communities.[Chang 2008a] The diagnosis of chronic suppurative lung disease is made in children who have symptoms and signs of bronchiectasis without radiographic features of bronchiectasis.[Chang 2008a] In Aboriginal and Torres Strait Islander children, it may be difficult to distinguish between asthma and bronchiectasis or chronic suppurative lung disease.[O’Grady 2010]
Protracted bacterial bronchitis is often misdiagnosed as asthma,[Craven 2013, Chang 2008b], but can also co-occur with asthma.[Chang 2008b] Inadequate treatment of protracted bacterial bronchitis might put Aboriginal and Torres Strait Islander children at risk for chronic suppurative lung disease.[Chang 2008b] Recurrent episodes of protracted bacterial bronchitis that does not resolve after treatment (e.g. a 14-day course of antibiotics) require investigation for chronic suppurative lung disease, bronchiectasis and aspiration.[Chang 2008b]
Chang AB, Masel JP, Boyce NC, et al. Non-CF bronchiectasis: clinical and HRCT evaluation. Pediatr Pulmonol 2003; 35: 477-483.
Chang AB, Grimwood K, Maguire G, et al. Management of bronchiectasis and chronic suppurative lung disease in indigenous children and adults from rural and remote Australian communities. Med J Aust 2008a; 189: 386-393.
Chang AB, Redding GJ, Everard ML. Chronic wet cough: Protracted bronchitis, chronic suppurative lung disease and bronchiectasis. Pediatr Pulmonol 2008b; 43: 519-531.
Morey MJ, Cheng AC, McCallum GB, Chang AB. Accuracy of cough reporting by carers of Indigenous children. J Paediatr Child Health 2013; 49: E199-203.
O’Grady KF, Revell A, Maguire G, et al. Lung Health Services for Aboriginal and Torres Strait Islander Peoples in Queensland. Queensland Health, Brisbane, 2010.
National cough guidelines: Cough in Children and Adults: Diagnosis, Assessment and Management (CICADA). Summary of an updated position statement on chronic cough in Australia.
Chronic suppurative lung disease is defined as a clinical syndrome of respiratory symptoms and signs due to chronic endobronchial suppuration, including continuous, wet or productive cough > 8 weeks, with or without other features (e.g. exertional dyspnoea, symptoms of reactive airway disease, recurrent chest infections, growth failure, clubbing, hyperinflation or chest wall deformity).[Chang 2010]
Bronchiectasis is diagnosed in patients with both chronic suppurative lung disease and the presence of radiological features on a chest high-resolution computed tomography scan.[Chang 2010]
If a provisional diagnosis of asthma can be made with high confidence, begin a treatment trial with a low dose of ICS (plus SABA as needed) for approximately 12 weeks.
If the diagnosis is uncertain, refer the child to an accredited respiratory function laboratory for diagnostic spirometry. If treatment is clinically urgent and delay to diagnostic spirometry is unacceptable, start treatment immediately. Ensure that parents receive the laboratory’s instructions on withholding of bronchodilators before the test.
Recommendation type: Consensus recommendation
Treatment trials for the purpose of confirming the diagnosis should be performed at a time when the child is likely to be exposed to usual triggers. A treatment trial is unlikely to provide evidence useful for supporting or ruling out the diagnosis if it is performed under conditions in which the child typically does not experience symptoms or have exacerbations (e.g. outside the cold and influenza season or when there is no relevant allergen exposure).
Spirometry to confirm the diagnosis should be conducted when possible.
Recommendation type: Consensus recommendation
National Asthma Council Australia’s Spirometry handbook for primary care
If spirometry is later conducted to confirm the diagnosis in a child receiving treatment for presumed asthma, the respiratory function laboratory may require withholding of bronchodilators.
Arrange either skin-prick testing or serum test for allergen-specific IgE.
Recommendation type: Consensus recommendation
Allergy testing is not recommended as a standalone diagnostic test for asthma, due to its low specificity.[ERS 2021] However, allergy testing at the time of diagnosis is useful to inform management because most children with asthma have allergies, which may affect asthma control.
The most common aeroallergens causing asthma or allergic rhinitis are dust mites, pollens (most often grass pollen, less often other wind-borne pollens from trees and weeds), animal epithelia, and moulds.[ASCIA 2020]
The history may help identify relevant aeroallergens for testing.
Either skin-prick testing or allergen-specific IgE antibody testing can be used to identify clinically relevant aeroallergens.[ASCIA 2024, ASCIA 2020]
ASCIA. Laboratory investigation for allergic diseases. Australasian Society of Clinical Immunology and Allergy, 2020.
ASCIA. Skin prick testing guide for diagnosis of allergic diseases. Australasian Society of Clinical Immunology and Allergy, 2024.
Gaillard EA, Kuehni CE, Turner S, et al. European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5-16 years. Eur Respir J 2021; 58: 2004173.
ASCIA’s Laboratory investigation for allergic diseases (2020)
ASCIA’s Skin prick testing guide for diagnosis of allergic diseases (2025)
Resources
The roles and interpretation of tests for type 2 inflammation in asthma, including fractional exhaled nitric oxide,…

Medication management
How to choose optimal starting treatment for children aged 6–11 years.