Australian Asthma Handbook
The National Guidelines for Health Professionals
Australian Asthma Handbook
The National Guidelines for Health Professionals
Cite
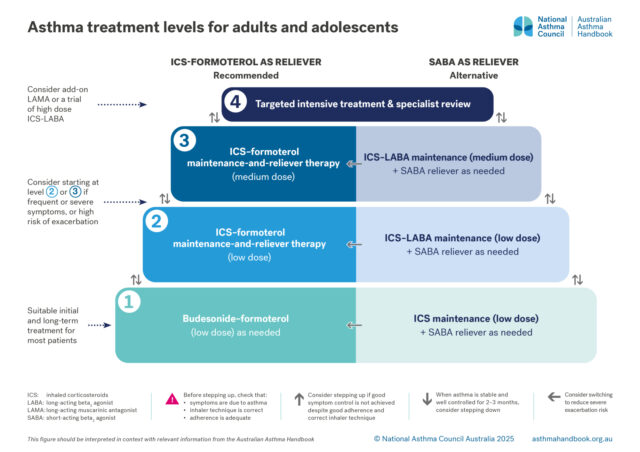
Step up or down one treatment level, or consider switching from a regimen with SABA as the reliever (alternative options) to a regimen with ICS-formoterol as the reliever (recommended options).
Recommendation type: Consensus
Prevention of exacerbations is a key goal of asthma management. Short courses of oral corticosteroids to manage asthma exacerbations are associated with increased lifetime risk of osteoporosis, pneumonia, cardiovascular or cerebrovascular diseases, cataract, sleep apnoea, renal impairment, depression/anxiety, type 2 diabetes, and weight gain. [Price 2018]
Most of the benefit of ICS is achieved at low doses. Long-term use of high doses increases the risk of systemic side-effects such as osteoporosis, cataract and glaucoma.[GINA 2025]
Observational data suggest that high daily doses of ICS are associated with an increased risk of adverse effects, including cataract, cardiovascular events, pulmonary embolism, and pneumonia,[Bloom 2024, von Bülow 2025] although these adverse events occur at low frequencies.[Bloom 2024] Even moderate daily doses have been associated with increased risk.[Bloom 2024]
Bloom CI, Yang F, Hubbard R, et al. Association of dose of inhaled corticosteroids and frequency of adverse events. Am J Respir Crit Care Med 2024; 211: 54–63.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy 2018; 11: 193-204.
von Bülow A, Hansen S, Sandin P, et al. Use of high-dose inhaled corticosteroids and risk of corticosteroid related adverse events in asthma -findings from the NORDSTAR cohort. J Allergy Clin Immunol Pract Feb 1: S2213-2198(25)00100-X.
Stepping up
Common causes of poor symptoms control or exacerbations include poor adherence, incorrect inhaler technique, exposure to triggers. Respiratory symptoms may also be due to a comorbid or alternative diagnosis (e.g. allergic rhinitis or rhinosinusitis, de-conditioning, obesity, heart disease, or inducible laryngeal obstruction).
Recommendation type: adapted from GINA
Poor inhaler technique is very common and is associated with poor asthma control, increased risk of exacerbations and increased adverse effects.[Melani 2011]
Low adherence to ICS treatment is very common among patients with asthma.[Murphy 2021]
Exposure to triggers (including viral upper respiratory tract infections, allergens or air pollution, including smoke) is a common cause of asthma symptoms and exacerbations.[GINA 2025]
Comorbidities can contribute to respiratory symptoms, exacerbations, or poor quality of life.[GINA 2025]
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med 2011; 105: 930-938.
Murphy J, McSharry J, Hynes L, et al. Prevalence and predictors of adherence to inhaled corticosteroids in young adults (15-30 years) with asthma: a systematic review and meta-analysis. J Asthma 2021; 58: 683-705.
Recommendation type: adapted from GINA
Low-dose budesonide-formoterol taken as needed is as effective as [O’Byrne 2018, Bateman 2018] or more effective than [Beasley 2019, Hardy 2019, Crossingham 2021] low-dose maintenance ICS (plus SABA as needed) for preventing severe exacerbations requiring oral corticosteroid treatment. The use of budesonide-formoterol as needed also results in a lower average ICS dose maintenance low-dose ICS plus SABA as needed.[O’Byrne 2018, Bateman 2018, Beasley 2019, Hardy 2019]
Bateman ED, Reddel HK, O'Byrne PM, et al. As-needed budesonide-formoterol versus maintenance budesonide in mild asthma. N Engl J Med 2018; 378: 1877-1887.
Beasley R, Holliday M, Reddel HK, et al. Controlled trial of budesonide-formoterol as needed for mild asthma. N Engl J Med 2019; 380: 2020-2030.
Crossingham I, Turner S, Ramakrishnan S, et al. Combination fixed-dose beta agonist and steroid inhaler as required for adults or children with mild asthma. Cochrane Database Syst Rev 2021; 5: CD013518.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Hardy J, Baggott C, Fingleton J, et al. Budesonide-formoterol reliever therapy versus maintenance budesonide plus terbutaline reliever therapy in adults with mild to moderate asthma (PRACTICAL): a 52-week, open-label, multicentre, superiority, randomised controlled trial. Lancet 2019; 394: 919-928.
O'Byrne PM, FitzGerald JM, Bateman ED, et al. Inhaled combined budesonide-formoterol as needed in mild asthma. N Engl J Med 2018; 378: 1865-1876.
For a patient using maintenance low-dose ICS-LABA plus SABA as needed (alternative Level 2 option), consider switching to low-dose MART.
For a patient using maintenance medium-dose ICS-LABA plus SABA as needed (alternative Level 3 option), consider switching to medium-dose MART (medium-dose maintenance ICS-formoterol plus as-needed low-dose ICS-formoterol).
Recommendation type: consensus recommendation
MART reduces the rate of exacerbations compared with fixed-dose maintenance ICS-LABA regimens (with SABA as needed) at the same or a higher ICS dose.[Sobieraj 2018]
Low-dose MART is associated with a reduction in severe exacerbations and a similar level of control, at relatively low ICS doses, compared with maintenance ICS-LABA plus as-needed SABA or a higher dose of ICS plus as-needed SABA.[Cates 2013, Kew 2013, Papi 2013, Patel 2013, Bateman 2011, Jorup 2018]
In patients with uncontrolled asthma on low-dose maintenance ICS-LABA plus SABA reliever, switching to MART reduced the rate of severe exacerbations, compared with stepping up to a higher dose of ICS-LABA maintenance plus SABA reliever. [Beasley 2022]
In RCTs in patients with uncontrolled asthma on medium-dose maintenance ICS-LABA plus SABA reliever:
The benefit of the MART regimen in reducing the risk of severe exacerbations requiring OCS appears to be due to the increase in doses of both the ICS and the formoterol at a very early stage of worsening asthma.[GINA 2025]
Bateman ED, Harrison TW, Quirce S, et al. Overall asthma control achieved with budesonide/formoterol maintenance and reliever therapy for patients on different treatment steps. Respiratory Res 2011; 12: 38.
Beasley R, Harrison T, Peterson S, et al. Evaluation of budesonide-formoterol for maintenance and reliever therapy among patients with poorly controlled asthma: a systematic review and meta-analysis. JAMA Netw Open 2022; 5: e220615.
Bousquet J, Boulet LP, Peters MJ, et al. Budesonide/formoterol for maintenance and relief in uncontrolled asthma vs. high-dose salmeterol/fluticasone. Respir Med 2007; 101: 2437-2446. Erratum in: Respir Med 2008; 102: 937-938.
Cates CJ, Karner C. Combination formoterol and budesonide as maintenance and reliever therapy versus current best practice (including inhaled steroid maintenance), for chronic asthma in adults and children. Cochrane Database Syst Rev 2013; 4: CD007313.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Jorup C, Lythgoe D, Bisgaard H. Budesonide/formoterol maintenance and reliever therapy in adolescent patients with asthma. Eur Respir J 2018; 51: 1701688.
Kew KM, Karner C, Mindus SM, et al. Combination formoterol and budesonide as maintenance and reliever therapy versus combination inhaler maintenance for chronic asthma in adults and children. Cochrane Database Syst Rev 2013; 12: CD009019.
Kuna P, Peters MJ, Manjra AI, Jorup C, Naya IP, Martínez-Jimenez NE, Buhl R. Effect of budesonide/formoterol maintenance and reliever therapy on asthma exacerbations. Int J Clin Pract 2007; 61: 725-36.
Papi A, Corradi M, Pigeon-Francisco C, et al. Beclometasone–formoterol as maintenance and reliever treatment in patients with asthma: a double-blind, randomised controlled trial. Lancet Respir Med 2013; 1: 23-31.
Patel M, Pilcher J, Pritchard A, et al. Efficacy and safety of maintenance and reliever combination budesonide/formoterol inhaler in patients with asthma at risk of severe exacerbations: a randomised controlled trial. Lancet Respir Med 2013; 1: 32-42.
Sobieraj DM, Weeda ER, Nguyen E, et al. Association of inhaled corticosteroids and long-acting beta-agonists as controller and quick relief therapy with exacerbations and symptom control in persistent asthma: A systematic review and meta-analysis. JAMA 2018; 319: 1485-1496.
This recommendation applies to patients with good adherence to ICS-containing treatment and correct inhaler technique, and after assessing and managing other risk factors such as comorbid conditions and exposure to avoidable triggers.
If asthma is not well controlled on medium-dose maintenance ICS-LABA plus SABA as needed, consider first switching to medium-dose MART first and monitoring control.
If specialist consultation is delayed, consider arranging spirometry by an accredited respiratory laboratory in the interim (see Difficult and severe asthma).
Recommendation type: Consensus recommendation
Raised blood eosinophil count and/or raised FeNO are characteristic of type 2 inflammation in asthma.
Patients with asthma with type 2 inflammation that does not respond to medium-dose ICS or higher are at high risk of exacerbations, and are likely to benefit from monoclonal antibody therapy.[GINA 2025]
Spirometry also guides consideration of add-on LAMA treatment, because the addition of LAMA to ICS-LABA is more likely to benefit adults with reduced lung function than those with normal lung function, independent of baseline blood eosinophil count.[Lee 2021].
More information: Lung function tests
More information: Tests for airway inflammation
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Lee LA, Bailes Z, Barnes N, et al. Efficacy and safety of once-daily single-inhaler triple therapy (FF/UMEC/VI) versus FF/VI in patients with inadequately controlled asthma (CAPTAIN): a double-blind, randomised, phase 3A trial. [Erratum in: Lancet Respir Med 2021; 9: e18.] Lancet Respir Med 2021; 9: 69-84.
Thoracic Society of Australia and New Zealand’s list of accredited respiratory laboratories.
Raised eosinophil count (≥150 cells/microlitre) in a patient taking medium-dose ICS or daily oral corticosteroids suggests refractory type 2 inflammation. Blood eosinophils may be elevated for reasons other than asthma. A very high blood eosinophil count ≥1500 cells/microlitre suggests other serious complications of asthma (e.g. allergic bronchopulmonary aspergillosis) or other serious conditions (e.g. eosinophilic granulomatosis with polyangiitis that require urgent specialist assessment).
Stepping down
Recommendation type: adapted from GINA
The aim of reducing the intensity of treatment when asthma is well controlled (good symptom control and low risk of exacerbations) are to find the optimal dose to control asthma and minimise side-effects.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Recommendation type: adapted from GINA
Low-dose budesonide-formoterol taken as needed is as effective as [O’Byrne 2018, Bateman 2018] or more effective than [Beasley 2019, Hardy 2019, Crossingham 2021] low-dose maintenance ICS (plus SABA as needed) for preventing severe exacerbations requiring oral corticosteroid treatment. The use of budesonide-formoterol as needed also results in a lower average ICS dose maintenance low-dose ICS plus SABA as needed.[O’Byrne 2018, Bateman 2018, Beasley 2019, Hardy 2019]
Bateman ED, Reddel HK, O'Byrne PM, et al. As-needed budesonide-formoterol versus maintenance budesonide in mild asthma. N Engl J Med 2018; 378: 1877-1887.
Beasley R, Holliday M, Reddel HK, et al. Controlled trial of budesonide-formoterol as needed for mild asthma. N Engl J Med 2019; 380: 2020-2030.
Crossingham I, Turner S, Ramakrishnan S, et al. Combination fixed-dose beta agonist and steroid inhaler as required for adults or children with mild asthma. Cochrane Database Syst Rev 2021; 5: CD013518.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Hardy J, Baggott C, Fingleton J, et al. Budesonide-formoterol reliever therapy versus maintenance budesonide plus terbutaline reliever therapy in adults with mild to moderate asthma (PRACTICAL): a 52-week, open-label, multicentre, superiority, randomised controlled trial. Lancet 2019; 394: 919-928.
O'Byrne PM, FitzGerald JM, Bateman ED, et al. Inhaled combined budesonide-formoterol as needed in mild asthma. N Engl J Med 2018; 378: 1865-1876.
Managing exacerbations
Include instructions in the patient’s written asthma action plan about:
Recommendation type: Consensus recommendation
Maximal reliever doses differ between relievers
See: Asthma exacerbations and acute asthma: definitions and classification
Give oral prednisone/prednisolone:
Recommendation type: Consensus recommendation
Management of worsening asthma symptoms must balance avoidance of adverse effects of systemic corticosteroids with risks of inadequately treated asthma exacerbations.
Prevention of exacerbations is a key goal of asthma management. Short courses of oral corticosteroids to manage asthma exacerbations are associated with increased lifetime risk of osteoporosis, pneumonia, cardiovascular or cerebrovascular diseases, cataract, sleep apnoea, renal impairment, depression/anxiety, type 2 diabetes, and weight gain.[Price 2018]
However, when the patient is already experiencing worsening asthma symptoms and is at risk of a severe exacerbation, prompt treatment with systemic corticosteroids is indicated to avoid emergency department attendance, hospitalisation, or life-threatening acute asthma.
Prednisone/prednisolone doses for adults are based on studies conducted in patients with asthma exacerbations presenting emergency departments.[Rowe 2001, Rowe 2007, Rowe 2017] Doses for adolescents are based on studies in children.[Normansell 2016, Chang 2008] Tapering the dose is not necessary for short courses.[O’Driscoll 1993]
Emphasise that the medicine only for severe exacerbations in the person for whom it was prescribed, and should not be used for any other purpose. Monitor frequency of oral corticosteroid use.
Chang, A B, Clark, R, Sloots, T P, et al. A 5- versus 3-day course of oral corticosteroids for children with asthma exacerbations who are not hospitalised: a randomised controlled trial. Med J Aust. 2008; 189: 306-310.
Normansell R, Kew KM, Mansour G. Different oral corticosteroid regimens for acute asthma. Cochrane Database Syst Rev 2016; Issue 5: CD011801.
O’Driscoll BR, Kalra S, Wilson M, et al. Double-blind trial of steroid tapering in acute asthma. Lancet 1993; 341: 324-327.
Price DB, Trudo F, Voorham J, et al. Adverse outcomes from initiation of systemic corticosteroids for asthma: long-term observational study. J Asthma Allergy 2018; 11: 193-204.
Rowe BH, Kirkland SW, Vandermeer B et al. Prioritizing systemic corticosteroid treatments to mitigate relapse in adults with acute asthma: a systematic review and network meta-analysis. Acad Emerg Med 2017; 24: 371-81.
Rowe BH, Spooner C, Ducharme F, et al. Early emergency department treatment of acute asthma with systemic corticosteroids. Cochrane Database Syst Rev 2001; Issue 1: CD002178.
Rowe BH, Spooner C, Ducharme F, et al. Corticosteroids for preventing relapse following acute exacerbations of asthma. Cochrane Database Syst Rev 2007; Issue 3: CD000195.
Instructions about when to start a short course of oral corticosteroids should also be included in the person’s written asthma action plan.
Prescribers should avoid supplying parents with more prednisone/prednisolone than needed for the course. Prescribers may write PBS scripts for less than the maximum quantity and number of repeats permitted if a lesser quantity is sufficient for the patient’s requirements.
The decision whether to provide a single script (no repeats) of prednisone/prednisolone and advise patients/parents to keep the medicine ready to use if instructed by the written asthma action plan, or only if instructed by a health professional after clinical assessment, depends on the patient’s age, ability to self-management, and access to a pharmacy.
For younger adolescents, assessment by a GP or virtual emergency consultation service is generally recommended before starting a short course of oral corticosteroids.
Information on managing acute asthma in adults & adolescents in primary care
Information on educating adults and adolescents to manage their asthma
Step up the regimen as necessary to regain or maintain control during pregnancy.
Recommendation type: Consensus recommendation
In Australia an estimated 12–13% of pregnant women have asthma.[Murphy 2023] Approximately 40% of pregnant women with asthma experience worsening asthma symptoms, and at least 20% have an exacerbation that requires medical intervention.[Murphy 2023]
Asthma exacerbations during pregnancy are associated with low birth weight, preterm birth, and small for gestational age status.[Murphy 2023] However, among women with asthma that is managed by a health professional, the risk of preterm labour and preterm delivery is not significantly higher than for non-asthmatic pregnant women.[Murphy 2011]
The Therapeutic Goods Administration database on prescribing medicines in pregnancy has assessed several asthma medicines as Category A or B3.[TGA] The TGA safety statement The benefits of asthma control outweigh any potential for an adverse pregnancy outcome applies to the following asthma medicines: budesonide, beclometasone, fluticasone furoate, fluticasone propionate, salmeterol.[TGA]
Murphy VE, Gibson PG, Schatz M. Managing asthma during pregnancy and the postpartum period. J Allergy Clin Immunol Pract 2023; 11: 3585-3594.
Murphy VE, Namazy JA, Powell H, et al. A meta-analysis of adverse perinatal outcomes in women with asthma. BJOG 2011; 118: 1314-1323.
TGA. Prescribing medicines in pregnancy database. The Australian categorisation system and database for prescribing medicines in pregnancy. [Website] [Accessed February 2025] Australian Government Department of Health and Aged Care Therapeutic Goods Administration
More information on asthma in pregnancy

Guide to asthma medicines, including types of treatment regimens, brand names, single-inhaler combinations, and inhaler…

Medication management
How to investigate asthma that is not well controlled despite treatment with medium-dose ICS-LABA

Adults and adolescents
How to conduct a rapid assessment and administer bronchodilators and supplementary oxygen to patients aged 12+ years…