Australian Asthma Handbook
The National Guidelines for Health Professionals
Australian Asthma Handbook
The National Guidelines for Health Professionals
Cite
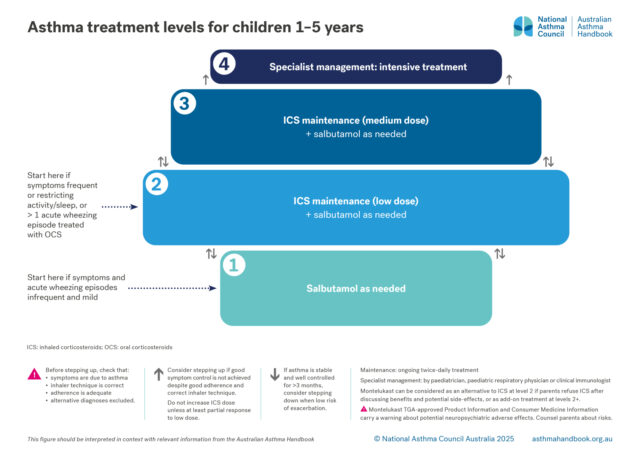
Asthma treatment is adjusted to maintain good control of asthma symptoms and prevent exacerbations, while minimising side-effects. The optimal step for an individual child may change over time. Remission may occur in some children.
There are four levels of treatment, from least intensive to most intensive.
Level 1. Salbutamol as needed
Level 2. Maintenance treatment with low-dose ICS (plus salbutamol as needed)
Level 3. Maintenance treatment with medium-dose ICS (plus salbutamol as needed)
Level 4. Specialist treatment
Specialist treatment at level 4 may include high-dose ICS or use of medicines approved for use in older children).
Specialists can include paediatricians, paediatric respiratory physicians and clinical immunologists.
Level 2: daily montelukast plus salbutamol as needed – can be considered if parents refuse ICS treatment after discussing benefits and risks. Switch to ICS when possible
Level 3: maintenance treatment with low-dose ICS plus montelukast, or (for children ≥4 years) maintenance treatment with low-dose ICS-LABA
Salbutamol
All children with asthma should be treated with salbutamol as needed when symptoms occur, delivered by pMDI plus spacer (with mask for those unable to form a tight lip seal around the spacer mouthpiece).
Salbutamol as needed can be considered as the sole asthma treatment for children with mild and infrequent symptoms and no history of a severe exacerbation or risk factors for severe exacerbations.
However, frequent use indicates that the child needs ICS treatment to reduce the risk of exacerbations. Consumption three or more canisters of salbutamol in a year indicates that the child’s asthma is poorly controlled. A large cohort study reported that, in children aged 1–5 years, prescription of three or more SABA canisters per year was associated with at least double the risk of subsequent exacerbations, compared with lower SABA prescribing.[Morgan 2023]
Maintenance low-dose ICS
In children aged 6 years and under with recurrent wheeze due to asthma, daily ICS treatment reduces the risk of exacerbations, compared with placebo and compared with daily montelukast.[Kaiser 2016]
The findings of a double-blind cross-over study children aged 1–5 years suggest that greater improvements in symptom control are typically achieved with daily low-dose ICS than daily montelukast.[Fitzpatrick 2016] Hypersensitivity to aeroallergens is associated with a higher probability of symptoms responding best to daily ICS treatment.[Fitzpatrick 2016] Raised blood eosinophil count, a marker of type-2 airway inflammation, is also associated with a higher probability of achieving best with daily ICS, compared with intermittent ICS or montelukast.[Fitzpatrick 2016] However, blood eosinophil count is not recommended as a routine test in assessing asthma in preschool children.
Maintenance low-dose ICS-LABA
ICS-LABA is approved by TGA for use in children ≥4 years.[Australian PI: fluticasone propionate-salmeterol]
Low-dose ICS-LABA is a treatment option for children aged 4 years and over, based on limited evidence from clinical trials of salmeterol added to ICS in children 5 years and younger reporting reductions in exacerbations and symptoms, compared with ICS alone or previous treatment, [Ambrożej 2024] and on efficacy studies in older children.[GINA 2025]
There is insufficient safety data to support the use of ICS-LABA in children younger than 4 years.[GINA 2025]
Safey considerations with ICS or ICS-LABA
Potential adverse effects must be weighed against benefits.
At recommended doses, ICSs are generally well tolerated in children.[Rachelefsky 2009; Kapadio 2016]
The use of a spacers with pMDIs reduces oropharyngeal drug deposition and therefore reduces the risk of local adverse effects (e.g. candidiasis and dysphonia) with ICS.[Lavorini 2020]
Topical effects of ICS can also be reduced by mouth-rinsing and spitting after inhaling. Immediate quick mouth-rinsing removes more residual medicine in the mouth than delayed rinsing.[Yokoyama 2007]
ICS-related systemic adverse effects in children include suppression of the hypothalamic-pituitary-adrenal (HPA) axis (rare),[Kapadio 2016] short-term linear growth suppression, clinically non-significant effects on bone mineral density, and dose-dependent effects on glucose metabolism.[Kapadio 2016]
A review of long-term clinical trials of recommended doses of inhaled corticosteroids in children found little or no effect on measures of HPA axis function over 12 to 36 months follow-up, and no clinically significant effects on bone mineral density.[Pedersen 2006]
Regular use of ICS in children before puberty is associated with an average reduction of 0.48 cm/year in linear growth rate in the first year of treatment, after which less effect is seen. Growth suppression depends on the dose.[Axelsson 2019]
Uncontrolled asthma also reduces children’s growth and final adult height.[Pedersen 2001]
In children aged 4–11 years, addition of LABA to ICS does not increase risk of exacerbations, contrary to historical concerns.[Stempel 2016]
Montelukast
Montelukast can be considered when parents refuse ICS treatment after discussing benefits and potential adverse effects.
Daily montelukast alone is generally ineffective for preventing exacerbations in children aged 1–5 years.[Valovirta 2011] However, a minority of children may benefit. The findings of a double-blind cross-over study children aged 1–5 years suggest that, while daily low-dose ICS typically achieves the greatest improvement in symptom control, some children’s symptoms show a stronger response to daily montelukast.[Fitzpatrick 2016] Clinical response to montelukast cannot be predicted by atopic status or biomarkers.[Fitzpatrick 2016]
Montelukast has been associated with neuropsychiatric disorders in all age groups and carries a warning label in Australia.[TGA 2025] The most commonly reported among children appear sleep disorders in infants aged <2 years and depression/anxiety in children aged 2–11 years.[Aldea Perona 2016]
Aldea Perona A, García-Sáiz M, Sanz Álvarez E. Psychiatric disorders and montelukast in children: a disproportionality analysis of the VigiBase®. Drug Saf 2016; 39: 69-78.
Ambrożej D, Cieślik M, Feleszko W, et al. Addition of long-acting beta-agonists to inhaled corticosteroids for asthma in preschool children: A systematic review. Paediatr Respir Rev 2024: S1526-0542(24)00079-4.
Australian Product Information – Pavtide (fluticasone propionate/ salmeterol xinafoate) Accuhaler and pMDI. [Revised 7 November 2022] Therapeutic Goods Administration (www.ebs.tga.gov.au)
Australian Product Information – Seretide (fluticasone propionate/ salmeterol xinafoate) Accuhaler and MDI. [Revised 7 November 2022] Therapeutic Goods Administration (www.ebs.tga.gov.au)
Axelsson I, Naumburg E, Prietsch SO, Zhang L. Inhaled corticosteroids in children with persistent asthma: effects of different drugs and delivery devices on growth. Cochrane Database Syst Rev 2019; 6: CD010126.
Fitzpatrick AM, Jackson DJ, Mauger DT, et al. Individualized therapy for persistent asthma in young children. J Allergy Clin Immunol 2016; 138: 1608-1618.e12.
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Kaiser SV, Huynh T, Bacharier LB, et al. Preventing exacerbations in preschoolers with recurrent wheeze: a meta-analysis. Pediatrics 2016; 137: e20154496.
Knorr B, Franchi LM, Bisgaard H, et al. Montelukast, a leukotriene receptor antagonist, for the treatment of persistent asthma in children aged 2 to 5 years. Pediatrics 2001; 108: E48.
Morgan A, Maslova E, Kallis C, et al. Short-acting β2-agonists and exacerbations in children with asthma in England: SABINA Junior. ERJ Open Res 2023; 9: 00571-2022.
Pedersen S. Do inhaled corticosteroids inhibit growth in children? Am J Respir Crit Care Med 2001; 164: 521-35.
Stempel DA, Szefler SJ, Pedersen S, et al. Safety of adding salmeterol to fluticasone propionate in children with asthma. N Engl J Med 2016; 375: 840-849.
Therapeutic Goods Administration. More prominent safety warnings about the neuropsychiatric effects of montelukast [Webpage] 16 January 2025.
Valovirta E, Boza ML, Robertson CF, et al. Intermittent or daily montelukast versus placebo for episodic asthma in children. Ann Allergy Asthm Immunol 2011; 106: 518-526.
Few medicines are approved for asthma treatment in children 1–5 years. Check TGA-approved indications for and PBS restrictions before prescribing.