Australian Asthma Handbook
The National Guidelines for Health Professionals
Australian Asthma Handbook
The National Guidelines for Health Professionals
Cite
Read first
Table
| Alternative or comorbid condition | Suggestive features |
| Inducible laryngeal obstruction | Dry cough or breathing difficulty triggered by strong smells, irritants or exercise Symptoms worse when talking on the phone Symptoms associated with throat tightness or voice change Breathlessness worst at peak exercise. Inspiratory wheezing (stridor) – strongly suggests a laryngeal or upper airway abnormality |
| Rhinosinusitis | Cough co-occurring with symptoms of rhinosinusitis |
| Chronic upper airway cough syndrome | Dry cough is dominant symptom Throat-clearing Dysphonia ‘Scratchy’ throat Triggered by talking, laughing, strong odours or smoke May be associated with chronic rhinosinusitis or gastroesophageal reflux |
| ACE inhibitor-related cough | Cough is dominant symptom |
| COPD | Onset of dyspnoea/cough/ wheeze at age >40 years History of smoking or exposure to smoke/dust History of recurrent chest infections Persistent breathlessness Family history of emphysema |
| Bronchiectasis | Productive cough in a patient with a history of recurrent infections |
| Large airway stenosis | Breathlessness or wheeze |
| Pulmonary fibrosis | Breathlessness or dry cough Fine crackles heard during inspiration on auscultation |
| Lung cancer | Persistent cough despite treatment Haemoptysis Chest pain Weight loss |
| Poor cardiopulmonary fitness | Breathlessness on exertion |
| Heart disease | Chest tightness on exertion Dyspnoea on exertion or when lying flat Basal crepitations |
| Pulmonary embolism | Sudden-onset dyspnoea |
| Dysfunctional breathing | Breathlessness with dizziness, light-headedness, or tingling fingers |
| Panic attacks | Breathlessness or chest tightness at rest or on minor exertion, accompanied by anxiety |
| Gastro-oesophageal reflux disease | Cough or chest tightness in patient with symptomatic reflux |
| Recurrent respiratory infections | As clinically typical |
Additional information
ACE: angiotensin-converting enzyme; COPD: chronic obstructive pulmonary disease
Table
Asthma is more likely to explain signs/symptoms More than one of these symptoms: wheeze, breathlessness, chest tightness, cough Symptoms recurrent or seasonal Symptoms worse at night or in the early morning History of allergies (e.g. allergic rhinitis, atopic dermatitis) Symptoms obviously triggered by exercise, cold air, irritants, certain medicines (e.g. aspirin or beta blockers), allergies, viral infections Family history of asthma or allergies Widespread wheeze audible on chest auscultation FEV1 or PEF lower than predicted, without other explanation Eosinophilia or raised blood IgE level, without other explanation Symptoms rapidly relieved by a rapid-acting bronchodilator (e.g. SABA or ICS-formoterol) |
Asthma is less likely to explain the signs/symptoms Dizziness, light-headedness, peripheral tingling Isolated cough with no other respiratory symptoms Chronic sputum production No abnormalities on physical examination of chest when symptomatic (over several visits) Change in voice Heavy smoker (now or in past) Cardiovascular disease Normal spirometry when symptomatic (despite repeated tests) |
Additional information
FEV1: forced expiratory volume in 1 second; ICS: inhaled corticosteroids; PEF: peak expiratory flow; Ig: immunoglobin; SABA: short-acting beta2 agonist
Ask about:
Recommendation type: Consensus recommendation
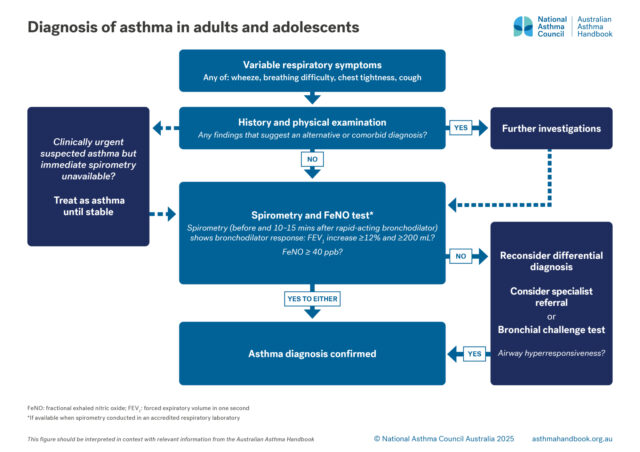
A history of fluctuating respiratory symptoms (e.g. wheeze, breathlessness, chest tightness, cough) is essential to the diagnosis of asthma. However, history alone is not adequate to confirm the diagnosis of asthma; the diagnosis also requires demonstration of variable expiratory airflow limitation.
Wheeze and dyspnoea are the symptoms most reliably associated with asthma.
Exercise-induced symptoms that worsen after stopping the activity strongly suggest asthma. Breathlessness due to other conditions (e.g. deconditioning, cardiac failure, COPD, inducible laryngeal obstruction) is usually worst during exertion.
Symptom patterns that suggest asthma include recurrence or seasonality of symptoms, worsening of symptoms at night or in the early morning, symptoms triggered by exercise, cold air, viral infections, allergies, or medicines (e.g. aspirin or beta-blockers).
Asthma should also be suspected in a patient with a history of recurrent episodes of ‘bronchitis’ or prolonged coughing after respiratory tract infections.
A family history of asthma or allergies increases the probability that typical respiratory symptoms are due to asthma.
Reddel HK. Common conditions that mimic asthma. Med J Aust. 2022; 216: 337-340.
Check for signs that suggest a comorbid or an alternative diagnosis, such as allergic rhinitis, rhinosinusitis, nasal polyps, heart murmurs, crackles or inspiratory wheeze.
Recommendation type: Consensus recommendation
The absence of detected abnormalities does not exclude a diagnosis of asthma. Physical examination is usually normal in an adult or adolescent with asthma.
Wheeze (if detected) does not confirm the diagnosis of asthma. Widespread wheeze on auscultation of the chest, when symptoms are present, suggests asthma but is nonspecific. Note: silent chest occurs in life-threatening asthma exacerbation.
Inspect the upper airway for signs of allergic rhinitis (e.g. swollen turbinates, transverse nasal crease, reduced nasal airflow, mouth breathing, darkness and swelling under eyes caused by sinus congestion).
Reddel HK. Common conditions that mimic asthma. Med J Aust. 2022; 216: 337-340.
If spirometry is not available within the practice, refer to an accredited respiratory function laboratory and request spirometry and FeNO in the same session.
Do not delay treatment, if indicated.
Bronchodilator responsiveness (whether respiratory airflow limitation is ‘reversible’) should be tested by measuring FEV1 before, and 10–15 minutes after, administration of a rapid-acting bronchodilator (e.g. salbutamol), with at least three spirometry manoeuvres each time.
Recommendation type: Recommendation adapted from GINA
Lung function testing is essential to distinguish asthma from other conditions including eosinophilic bronchitis, allergic rhinitis, inducible laryngeal obstruction and COPD.
Spirometry, when correctly performed, is the most accurate and reliable test for assessing lung function in a patient with suspected asthma.
Reduced ratio of FEV1 to FVC indicates expiratory airflow limitation. Decreased FEV1 alone is a nonspecific finding and does not confirm asthma.
Normal spirometry does not exclude asthma, especially when patient is asymptomatic.
A positive bronchodilator response (increase ≥12% and ≥ 200 mL from pre-bronchodilator FEV1) confirms the diagnosis of asthma if the clinical history and physical examination findings are consistent with asthma.
TSANZ’s list of accredited respiratory function laboratories
National Asthma Council Australia’s spirometry training and tools
If high-quality spirometry cannot be performed in a primary care practice, refer the patient to an accredited respiratory function laboratory.
When interpreting a bronchodilator responsiveness test, the greater the increase in FEV1, the more likely the diagnosis of asthma. An increase from baseline >400 mL strongly supports the diagnosis of asthma.
A bronchodilator response that does not meet criteria for a positive test does not rule out asthma. If the post-bronchodilator increase in FEV1 approaches, but does not reach, the criteria for positive response, this information must be interpreted alongside other findings.
Alternative criteria for positive bronchodilator responsiveness test are used in some respiratory function laboratories and guidelines, and may be incorporated into spirometer software.
Patients with longstanding asthma may develop persistent expiratory airflow limitation, defined as FEV1/FVC <0.7 or < lower limit of normal.[Rutting 2022] Among this group, approximately two-thirds have a negative bronchodilator response on spirometry.[Rutting 2022]
More information: Lung function tests
Recommendation type: Consensus recommendation
FeNO is elevated in the presence of active type-2 inflammation of the airway associated with asthma.
FeNO ≥40 ppb supports the diagnosis of asthma in a patient with spirometry indicating expiratory airflow limitation and signs and symptoms strongly suggesting asthma. In adults, a FeNO level ≥ 40 ppb in adults has a reported sensitivity of 0.61 and specificity of 0.82 and for the diagnosis of asthma [Louis 2022]
Normal FeNO does not rule out asthma.[Louis 2022, Karrasch 2017]
Karrasch S, Linde K, Rücker G, et al. Accuracy of FENO for diagnosing asthma: A systematic review. Thorax 2017; 72: 109–116.
Louis R, Satia I, Ojanguren I, et al. European Respiratory Society guidelines for the diagnosis of asthma in adults. Eur Respir J 2022; 60: 2101585.
More information on tests for airway inflammation
Recommendation type: Adapted from GINA
In adults and adolescents with recent-onset respiratory symptoms (months to years), the diagnosis of asthma is confirmed by documenting both a history of typical symptoms and demonstration of excessive variability of expiratory airflow (including historical documentation).
Variable airflow can be demonstrated several ways, including:
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Rutting S, Thamrin C, Cross TJ, et al. Fixed airflow obstruction in asthma: a problem of the whole lung not of just the airways. Front Physiol 2022; 13: 898208.
Alternative criteria for bronchodilator response are used in some spirometry software and testing centres.[Stanojevic 2021]
Patients with longstanding asthma may develop persistent expiratory airflow limitation, defined as FEV1/FVC <0.7 or < lower limit of normal.[Rutting 2022] Among this group, approximately two-thirds have a negative bronchodilator response on spirometry.[Rutting 2022]
Consider:
Recommendation type: Recommendation adapted from GINA and ERS
Repeating spirometry within the practice (e.g. when the patient has symptoms or early in the morning)[GINA 2025] or referring to an accredited respiratory laboratory may provide more diagnostic information because spirometry results vary with the patient’s clinical status at the time of testing and with the quality of spirometry.
FeNO is elevated in the presence of active type-2 inflammation of the airway associated with asthma. A high FeNO level supports the diagnosis of asthma in a patient with symptoms suggesting asthma.[Louis 2022] Normal FeNO does not rule out asthma.[Louis 2022]
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Louis R, Satia I, Ojanguren I, et al. European Respiratory Society guidelines for the diagnosis of asthma in adults. Eur Respir J 2022; 60: 2101585.
Rutting S, Thamrin C, Cross TJ, et al. Fixed airflow obstruction in asthma: a problem of the whole lung not of just the airways. Front Physiol 2022; 13: 898208.
More information on tests for airway inflammation
More information on lung function testing
Recommendation type: Consensus recommendation
Bronchial provocation (challenge) tests for airway hyperresponsiveness are not required for asthma diagnosis, but can be considered if the bronchodilator responsiveness test is negative on initial spirometry.
If pre-bronchodilator lung function is normal, bronchial provocation testing is unlikely to detect significant airway hyperresponsiveness.
More information: Lung function tests
Bronchial provocation (challenge test) involves measuring lung function before and after a standardised challenge calculated to provoke bronchoconstriction in a controlled, closely monitored test.
Bronchial provocation tests are performed only in accredited respiratory function laboratories.
Types of bronchial provocations tests include methacholine challenge, mannitol challenge, exercise challenge, and eucapnic voluntary hyperventilation. Optimal selection depends on the patient’s age and on the provisional and differential diagnoses based on the clinical findings and results of other investigations.
If the patient is using bronchodilator medication, check the respiratory laboratory’s requirements for withholding bronchodilators before the test.
Standard withholding times are:
Bronchial provocation testing is not possible in a patient who cannot perform spirometry.
More information on lung function testing
Recommendation type: Consensus recommendation
Instruct the patient to keep a PEF diary for 2–4 weeks: every morning on waking and every afternoon at approximately 4 pm, the patient takes three PEF readings and records the highest of three. Use the data to calculate mean daily variation.
Recommendation type: Adapted from GINA
The best method for testing lung function in a patient with suspected asthma is spirometry performed by a trained operator with suitable equipment, with bronchodilator responsiveness testing. However, if spirometry is not accessible within a few weeks or days (according to clinical urgency), consider PEF measurement in preference to no lung function test.
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Asthma + Lung UK’s Peak flow variability calculator
Mean diurnal variability is calculated as follows: [GINA 2025]
1. Calculate each day’s score: ( [day’s highest – day’s lowest] / mean of day’s highest and lowest) x 100
2. Add up each daily score over the monitoring period and calculate the mean.
Daily variation >10% supports the diagnosis of asthma.
An online calculator using the daily amplitude percent mean method is available from Asthma + Lung UK.
Recommendation type: Consensus recommendation
Recommendation type: Adapted from GINA
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Information on managing acute asthma in adults and adolescents in primary care and in emergency departments
If immediate referral is not possible, arrange spirometry with bronchodilator responsiveness testing, and bronchial provocation testing if indicated.
Recommendation type: Adapted from TSANZ-NAC
New-onset asthma in an adult could be work-related asthma (work-exacerbated asthma or occupational asthma).
Investigation of suspected work-related asthma is complex. It involves systematically confirming the diagnosis of asthma, establishing the link between asthma symptoms and the workplace, and identifying the specific causal agent(s) through a detailed history, further investigations (e.g. serial PEF measurement, skin prick tests, bronchial provocation testing) and sometimes worksite visits.[Hoy 2020]
For patients with occupational asthma, prompt diagnosis and identification of causal exposures is critical to avoid rapid and potentially irreversible decline in lung function.[Hoy 2020]
Hoy R, Burdon J, Chen L, et al. Work-related asthma: A position paper from the Thoracic Society of Australia and New Zealand and the National Asthma Council Australia. Respirology 2020; 25: 1183-1192.
National Asthma Council Australia’s Work-related asthma. An update for primary care health professionals
National Asthma Council Australia and TSANZ’s position paper on work-related asthma
OASYS free software for diagnosis of occupational asthma using serial peak flow records
Work-related asthma includes occupational asthma and work-exacerbated asthma.
Occupational asthma is new-onset asthma (or recurrence of asthma after a period of remission) due to exposures to irritants or sensitisers in the workplace. Sensitiser-induced occupational asthma is far more common than irritant-induced occupational asthma.[Hoy 2020]
More information on work-related asthma
Consider referring to a respiratory physician or allergist/clinical immunologist.
Recommendation type: Consensus recommendation
Aspirin-exacerbated respiratory disease is a distinct condition resulting in adult-onset asthma.[Rajan 2015] It is present in approximately 7% of people with asthma and approximately 15% of people with severe asthma.[Rajan 2015]
Aspirin-exacerbated respiratory disease typically progresses from nasal congestion and anosmia to chronic rhinosinusitis with nasal polyps, then asthma and hypersensitivity to aspirin and NSAIDs.[Szczeklik 2000]
Within minutes to hours of ingesting aspirin or NSAIDs, people with aspirin-exacerbated respiratory disease can develop dyspnoea and other reactions that can include angioedema and anaphylactoid shock.[Szczeklik 2000]
A presumptive diagnosis of aspirin-exacerbated respiratory disease is based on a history of reactions to aspirin or nonselective NSAIDs, with a higher degree of certainty in patients with chronic rhinosinusitis and nasal polyps.[Kennedy 2016] Aspirin challenge, performed in a specialist clinic with cardiopulmonary resuscitation capabilities, provides a definitive diagnosis.[GINA 2025]
Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention, 2025. Available from: www.ginasthma.org
Kennedy JL, Stoner AN, Borish L. Aspirin-exacerbated respiratory disease: Prevalence, diagnosis, treatment, and considerations for the future. Am J Rhinol Allergy 2016; 30: 407-413.
Rajan JP, Wineinger NE, Stevenson DD, White AA. Prevalence of aspirin-exacerbated respiratory disease among asthmatic patients: A meta-analysis of the literature. J Allergy Clin Immunol 2015; 135: 676-81.
Szczeklik A, Nizankowska E, Duplaga M. Natural history of aspirin-induced asthma. AIANE Investigators. European Network on Aspirin-Induced Asthma. Eur Respir J 2000; 16: 432-436.
Recommendation type: Adapted from GINA
Bronchial provocation testing is contraindicated during pregnancy.[GINA 2025]
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
More information on asthma in pregnancy
Recommendation type: Consensus recommendation
An estimated 10% of Australian adolescents aged 14–17 years smoke or vape, and some parents are not aware of their child’s use of vapes.[Egger 2024a, Egger 2024b]
Egger S, David M, Watts C, et al. The association between vaping and subsequent initiation of cigarette smoking in young Australians from age 12 to 17 years: a retrospective cohort analysis using cross-sectional recall data from 5114 adolescents. Aust N Z J Public Health 2024; 48: 100173.
Egger S, Watts C, Dessaix A, et al. Parent's awareness of, and influence on, their 14-17-year-old child's vaping and smoking behaviours; an analysis of 3242 parent-child pairs in Australia. Addict Behav 2024; 150: 107931.
Royal Australasian College of Physicians. Routine adolescent and young adult psychosocial and health assessment. Position statement 2021. Sydney; RACP: 2021.
RACP’s position statement on psychosocial and health assessment for adolescents and young adults
More information on smoking and vaping
Use age-adjusted spirometry and FeNO reference values.
Recommendation type: Consensus recommendation
New cases of adult-onset asthma can occur at any age.[Gibson 2010]
Older adults with late-onset asthma may have typical signs and symptoms, or may present with cough as the only symptom.[Dunn 2018]
FEV1/FVC ratio decreases with aging, so age-adjusted reference values should be used to avoid overdiagnosis of airflow limitation.[Dunn 2018]
FeNO values in healthy individuals decrease from young adulthood and are markedly low in healthy older adults than young adults.[Högman 2024]
Dunn RM, Busse PJ, Wechsler ME. Asthma in the elderly and late-onset adult asthma. Allergy 2018; 73 : 284-294.
Gibson PG, McDonald VM, Marks GB. Asthma in older adults. Lancet 2010; 376: 803-813.
Högman M, Bowerman C, Chavez L, et al. ERS technical standard: Global Lung Function Initiative reference values for exhaled nitric oxide fraction (FENO50 ). Eur Respir J 2024; 63: 2300370.
Some older adults may not experience dyspnoea, even with significant airflow limitation.
Differential diagnosis includes other chronic diseases common in older patients (e.g. heart failure).[Dunn 2018]
Table: Differential diagnosis in adults and adolescents
For older adults with asthma-like symptoms, consider past history as well as current symptoms when interpreting findings, and do not rule out asthma immediately when bronchodilator responsiveness test is negative or symptoms are not typical.
Consider the possibility of COPD as an alternative diagnosis, and the possibility of both COPD and asthma as coexisting diagnoses.
Recommendation type: Adapted from GINA
In patients aged 60 years and over with new-onset respiratory signs/symptoms, consider a past diagnosis of asthma or historical symptoms to distinguish asthma (or coexisting asthma and COPD) from COPD.
Patients with longstanding asthma may develop persistent expiratory airflow limitation, defined as FEV1/FVC <0.7 or < lower limit of normal.[Rutting 2022] Among this group, approximately two-thirds have a negative bronchodilator response on spirometry [Rutting 2022] (sometimes called fixed airway limitation). These findings, which are mainly due to airway remodelling,[Rutting 2022] are also features of COPD.
People with features of both asthma and COPD must be distinguished from those with COPD, because ICS treatment is routinely indicated in those with asthma (in addition to bronchodilator therapy with LABA and/or LAMA).[GINA 2024] Patients with a past history of asthma or past diagnosis of asthma are at significantly greater risk of hospitalisation or death if they are treated with long-acting bronchodilators alone, than if they also receive ICS.[Gershon 2014, Kendzerska 2019, Suissa 2018]
Gershon AS, Campitelli MA, Croxford R, et al. Combination long-acting β-agonists and inhaled corticosteroids compared with long-acting β-agonists alone in older adults with chronic obstructive pulmonary disease. JAMA 2014; 312: 1114-1121.
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Kendzerska T, Aaron SD, To T, et al. Effectiveness and safety of inhaled corticosteroids in older individuals with chronic obstructive pulmonary disease and/or asthma. A population study. Ann Am Thorac Soc 2019; 16: 1252-1262.
Rutting S, Thamrin C, Cross TJ, et al. Fixed airflow obstruction in asthma: a problem of the whole lung not of just the airways. Front Physiol 2022; 13: 898208.
Suissa S, Ernst P. Observational studies of inhaled corticosteroid effectiveness in COPD: Lessons learned. Chest 2018; 154: 257-265.
Lung Foundation Australia’s The COPD-X Plan: Australian and New Zealand guidelines for the management of chronic obstructive pulmonary disease 2024
More information on COPD and asthma
Recommendation type: consensus
Heart failure is a common cause of persistent dyspnoea in older patients.[Reddel 2022]
The possibility of heart failure should be considered in patients with a history of cardiovascular disease (e.g. hypertension, valvular disease or ischaemic heart disease).[Reddel 2022]
ACE inhibitor-induced cough should also be considered.
Reddel HK. Common conditions that mimic asthma. Med J Aust 2022; 216: 337-340.
Reddel HK. Common conditions that mimic asthma. Med J Aust 2022; 216: 337-340.
Consensus recommendation
Historically, the prevalence of bronchiectasis has been disproportionately high in remote Aboriginal communities, particularly in Central Australia, but has been underdiagnosed.[Chang 2003, Chang 2008] High-resolution computed tomography of the chest is necessary to diagnose bronchiectasis in adults.[Chang 2008] In Aboriginal and Torres Strait Islander adults, it may be difficult to distinguish between asthma, COPD and bronchiectasis.[O’Grady 2010] Bronchiectasis is associated with relatively rapid decline in lung function.[Chang 2008]
Chang AB, Masel JP, Boyce NC, et al. Non-CF bronchiectasis: clinical and HRCT evaluation. Pediatr Pulmonol 2003; 35: 477-83.
Chang AB, Grimwood K, Maguire G, et al. Management of bronchiectasis and chronic suppurative lung disease in indigenous children and adults from rural and remote Australian communities. Med J Aust 2008a; 189: 386-93.
O’Grady KF, Revell A, Maguire G, et al. Lung health services for Aboriginal and Torres Strait Islander Peoples in Queensland. Queensland Health, Brisbane, 2010.
TSANZ’s position statement Cough in children and adults: diagnosis, assessment and management (2024)
Chronic suppurative lung disease is defined as a clinical syndrome of respiratory symptoms and signs due to chronic endobronchial suppuration, including continuous, wet or productive cough > 8 weeks, with or without other features (e.g. exertional dyspnoea, symptoms of reactive airway disease, recurrent chest infections, growth failure, clubbing, hyperinflation or chest wall deformity).[Chang 2010]
Bronchiectasis is diagnosed in patients with both chronic suppurative lung disease and the presence of radiological features on a chest high-resolution computed tomography scan.[Chang 2010]
If possible, refer competing athletes to a sports medicine expert or specialist with expertise in the investigation and management of asthma and exercise-induced bronchoconstriction in competitive athletes, to ensure that all investigations and treatments comply with requirements of sports governing bodies.
Do not rely on history alone to diagnose or exclude exercise-induced bronchoconstriction.
Recommendation type: Consensus recommendation
Asthma is common among elite sportspeople.[Hostrup 2024]
Exercise-induced bronchoconstriction can occur in athletes with or without asthma.[Greiwe 2020]
For some sports or levels of competition, governing bodies stipulate a specific testing protocol to demonstrate asthma before the athlete is permitted to use certain medicines.
Greiwe J, Cooke A, Nanda A, et al. Work Group Report: Perspectives in diagnosis and management of exercise-induced bronchoconstriction in athletes. J Allergy Clin Immunol Pract 2020; 8: 2542-2555.
Hostrup M, Hansen ESH, Rasmussen SM, Jessen S, Backer V. Asthma and exercise-induced bronchoconstriction in athletes: Diagnosis, treatment, and anti-doping challenges. Scand J Med Sci Sports 2024; 34:e14358.
Sport Integrity Australia’s information on asthma medication in sport
World Anti-Doping Agency guidelines for physicians on therapeutic use exemption for asthma
More information on exercise and asthma
Recommendation type: Consensus recommendation
Blood eosinophil count is not recommended as a primary diagnostic test for asthma.[ERS 2022]
Although an elevated blood eosinophil count is not necessary for the diagnosis of asthma, this finding may reflect airway inflammation. A high blood eosinophil count supports the diagnosis of asthma in a patient with acute symptoms consistent with asthma.
However, there is a risk of false positives and false negatives when fixed cut-points are used for blood eosinophils because people without asthma may have raised counts, and blood eosinophil count may be normal in a patient with asthma.[Blakey 2025]
Blakey JD, Ramakrishnan S. Using an eosinophil count to diagnose asthma: music to your EARS? Respirology 2025; 30: 280-282.
Louis R, Satia I, Ojanguren I, et al. European Respiratory Society guidelines for the diagnosis of asthma in adults. Eur Respir J 2022; 60: 2101585.
More information on tests for airway inflammation
Arrange skin-prick testing or allergen-specific blood immunoglobulin E assay for common aeroallergens, as guided by the history.
Recommendation type: Consensus recommendation
Allergic asthma generally accounts for less than 50% of cases of new-onset asthma in adults.[Pakkasela 2020]
Allergic sensitisation is not necessary for the diagnosis of asthma. Allergy testing does not rule asthma in or out. However, identifying clinically relevant airborne allergic triggers is useful to guide management.
Either spin-prick testing or allergen-specific IgE antibody testing can be used to identify clinically relevant aeroallergens.[ASCIA 2024, ASCIA 2020]
ASCIA. Laboratory investigation for allergic diseases. Australasian Society of Clinical Immunology and Allergy, 2020.
ASCIA. Skin prick testing guide for diagnosis of allergic diseases. Australasian Society of Clinical Immunology and Allergy, 2024.
Pakkasela J, Ilmarinen P, Honkamäki J, et al. Age-specific incidence of allergic and non-allergic asthma. BMC Pulm Med 2020; 20: 9.
ASCIA’s Laboratory investigation for allergic diseases (2020)
ASCIA’s Skin prick testing guide for diagnosis of allergic diseases (2025)
More information on allergies and asthma
Specific populations and clinical settings
Resources
Lung function testing
Resources
If the patient experiences symptoms during the withholding period they should follow their action plan. If reliever is necessary to manage symptoms, the test should be postponed
Other investigations
Making the diagnosis

Adults and adolescents
Why and how to confirm a previous asthma diagnosis, including when the patient is using asthma medicines.
The roles and interpretation of tests for type 2 inflammation in asthma, including fractional exhaled nitric oxide,…

The roles of spirometry, peak expiratory flow measurement, bronchial challenge testing, and oscillometry.

Clinical Topics
How to investigate asthma due to suspected triggers in the workplace.

Clinical Topics
Information on distinguishing asthma from COPD, and identifying and managing asthma in patients with features of COPD.

Clinical Topics
Information on links between asthma and allergies, management of allergic asthma, and management of allergic rhinitis…

Clinical Topics
Information on exercise-induced asthma symptoms in children and adults and asthma management for elite athletes.