Australian Asthma Handbook
The National Guidelines for Health Professionals
Australian Asthma Handbook
The National Guidelines for Health Professionals
Cite
Table
| Feature | Consider: |
| Symptoms present from birth | Cystic fibrosis Structural abnormality Bronchopulmonary dysplasia Primary ciliary dyskinesia |
| Abnormal voice | Acute viral laryngitis Vocal cord nodules Structural abnormalities Inducible laryngeal obstruction |
| Sudden breathlessness at rest | Panic attacks |
| Cough | |
| Acute onset | Inhaled foreign body |
| Dry cough occurring during daytime only | Somatic cough (previously called ‘habit’ cough) |
| Persistent productive cough | Bronchiectasis Cystic fibrosis Primary ciliary dyskinesia Protracted bacterial bronchitis |
| Persistent cough | Post-viral cough Allergic rhinitis Primary ciliary dyskinesia Pertussis |
| 🚩Cough with haemoptysis | Infection Inhaled foreign body Congestive heart disease Vascular abnormality Bronchial mass Cystic fibrosis |
| Upper respiratory tract | |
| Chronic production of sputum | Protracted bacterial bronchitis |
| Nasal polyps | Cystic fibrosis |
| Chest sounds | |
| 🚩 Unilateral wheeze | Inhaled foreign body |
| No variation in wheeze | Structural abnormality |
| Inspiratory wheeze | Inducible laryngeal obstruction |
| Sudden wheeze at rest | Panic attacks |
| Exercise-induced wheeze that stops immediately when exertion ceases | Inducible laryngeal obstruction Anxiety |
| Stridor | Croup Inducible laryngeal obstruction |
| Localised crepitation | Pneumonia |
| Cardiac murmur | Congenital heart disease |
| Skin and integument | |
| Finger clubbing | Cystic fibrosis Primary ciliary dyskinesia Bronchiectasis Immunodeficiency |
| Systemic signs | |
| Weight loss/lack of weight gain | Immunodeficiency |
| Fevers | Chronic infection |
| Growth failure | Cystic fibrosis Immunodeficiency |
| Recurrent or atypical infections | Immunodeficiency |
Additional information
These findings require further investigation or specialist referral. Flag symbol 🚩 indicates urgent referral needed.
Table
| Asthma more likely | Asthma less likely |
More than one of the typical asthma signs/symptoms: wheeze, difficulty breathing, feeling of tightness, in the chest, cough Signs/symptoms frequent Signs/symptoms worse at night and in the early morning Signs/symptoms triggered by exercise, exposure to pets, cold air, damp air, emotions, laughing Signs/symptoms occur when child doesn’t have a cold History of allergies (e.g. allergic rhinitis, atopic dermatitis, food allergies) Family history of allergies Family history of asthma Widespread wheeze heard on auscultation Signs/symptoms respond to treatment trial of reliever, with or without a preventer Lung function measured by spirometry increases in response to rapid-acting bronchodilator Lung function measured by spirometry increases in response to a treatment trial with inhaled corticosteroid (where indicated) | Symptoms only occur when child has a cold, but never between colds* Isolated cough in the absence of wheeze or difficulty breathing History of moist cough Exercise-induced dyspnoea with noisy inspiration Chest pain Dizziness, light-headedness or peripheral tingling Repeatedly normal physical examination of chest when symptomatic Focal wheeze Normal spirometry when symptomatic (children old enough to perform spirometry) No response to a trial of asthma treatment with adequate dose and correct inhaler technique Clinical features that suggest an alternative diagnosis |
Additional information
* In preschool children, wheezing that only occurs during viral respiratory infections may not be due to asthma, but this finding does not rule out asthma. Viral respiratory infection is the most common trigger for severe acute asthma exacerbations in children of all ages.
Ask about:
Recommendation type: Consensus recommendation
History features that suggest an alternative diagnosis, including red flags, are listed in Table: Signs and symptoms that suggest an alternative diagnosis in children
The probability of asthma is higher if signs and symptoms are frequent, triggered by common asthma triggers, sometimes occur in the absence of upper respiratory tract infections, or there is a family history of allergies or asthma (Table: Features suggesting higher or lower probability of asthma in children)
Royal Children’s Hospital Melbourne’s What is asthma? video for parents explaining how to identify wheeze and other signs
Include the following:
Recommendation type: Consensus recommendation
Physical examination findings that suggest an alternative diagnosis, including red flags, are listed in Table: Signs and symptoms that suggest an alternative diagnosis in children.
Usually no abnormalities are detected on physical examination of a child with asthma.
Objective confirmation of wheeze is useful. Check medical records for wheeze confirmed by a health professional. If wheeze is not detectable during the consultation, ask parents to record an episode (video or audio).
The chest may be silent in severe acute asthma.
Royal Children’s Hospital Melbourne’s What is asthma? video for parents explaining how to identify wheeze and other signs
Clinical response can be verified by either of the following:
Consensus recommendation
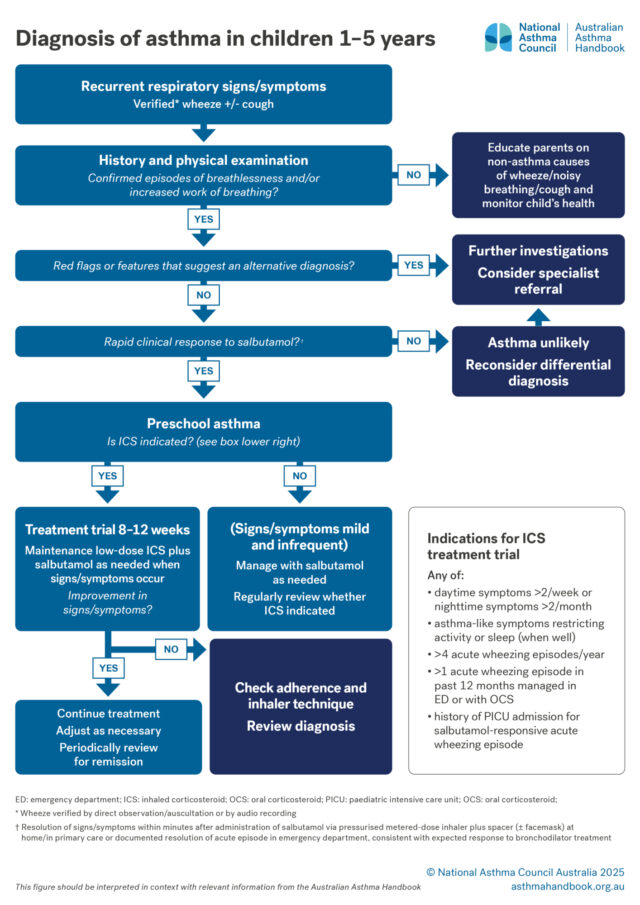
If symptoms rapidly and consistently resolve after administration of inhaled salbutamol, this supports the diagnosis of asthma.
A treatment trial with ICS is indicated for children with any of the following:
Recommendation type: Consensus recommendation
Resolution or significant improvement of signs and symptoms during a treatment trial with low-dose ICS supports the diagnosis of asthma.
If symptoms do not resolve during a trial of low-dose maintenance ICS, check inhaler technique, adherence, triggers, reconsider the diagnosis, and consider specialist referral.
The treatment trial should be performed at a time when the child is likely to be exposed to usual triggers.
A treatment trial is unlikely to provide evidence useful for supporting or ruling out the diagnosis if it is performed under conditions in which the child typically does not experience symptoms or have exacerbations (e.g. outside the cold and influenza season or when there is no relevant allergen exposure).
Recommendation type: Consensus recommendation
If a child younger than 12 months shows persistent wheezing, refer to a specialist.
Recommendation type: Consensus recommendation
In children younger than 12 months, episodes of acute wheeze with increased work of breathing are usually caused by bronchiolitis, which is most commonly due to respiratory syncytial virus.[Dalziel 2022]
Transient early wheeze (noisy breathing in infants younger than 12 months who are otherwise well and thriving) should not be diagnosed as asthma or treated with bronchodilators.
Dalziel SR, Haskell L, O'Brien S, et al. Bronchiolitis. Lancet 2022; 400: 392-406.
Suitable specialists for referral include paediatricians, paediatric respiratory physicians, and allergists.
Confirm that more than one episode has occurred.
Confirm that the sound reported by the child or parents is actually wheeze – ask parents to video/audio record the wheeze to verify.
Determine whether wheeze only occurs during viral respiratory tract infections, or also occurs during physical activity and at other times.
Recommendation type: Consensus recommendation
Careful questioning or recordings may be necessary to correctly identify respiratory signs. Parents may not be able to recognise wheezing, stridor, snoring or normal breathing. [Fernandes 2011]
Asthma is more likely if wheezing occurs during play or exposure to allergens.
Fernandes RM, Robalo B, Calado C, et al. The multiple meanings of "wheezing": a questionnaire survey in Portuguese for parents and health professionals. BMC Pediatr 2011; 11: 112.
Royal Children’s Hospital Melbourne’s What is asthma? video for parents explaining how to identify wheeze and other signs
Recommendation type: Consensus recommendation
Coughing is normal in preschool children in the context of frequent respiratory infections. Isolated dry cough in an otherwise well preschool child is rarely due to a specific diagnosis.[Bush 2023] Intermittent wet cough during viral colds is normal; preschool children typically have many colds per year with symptoms lasting up to 3 weeks each time.[Bush 2023]
Asthma is among the most common causes of chronic cough in children with no abnormality detected on physical examination, chest radiography or spirometry.[Marchant 2024] Asthma may cause episodic cough that is associated with expiratory wheeze and/or exertional dyspnoea.[Marchant 2024]
In children, cough due to asthma typically resolves within one month of treatment with ICS.[Marchant 2024] ICS treatment is not indicated unless there are specific features to suggest asthma.[Marchant 2024]
Chronic cough in the absence of other symptoms/signs is rarely due to asthma.[Marchant 2024] The diagnosis of preschool asthma should not be made unless the child also has breathlessness, chest tightness, or wheeze.[Bush 2023] Other causes of chronic cough in children include respiratory tract infections, airway anomaly, aspiration, rhinitis/rhinosinusitis and somatic syndrome.[Marchant 2024, Kantar 2022] Wet cough persisting beyond 3 weeks suggests protracted bacterial bronchitis requiring antibiotic treatment. Specialist referral should be considered for children with multiple episodes of prolonged wet cough or failure to resolved with antibiotic treatment.[Marchant 2024]
Bush A. Basic clinical management of preschool wheeze. Pediatr Allergy Immunol 2023; 34: e13988.
Kantar A, Marchant JM, Song WJ, et al. History taking as a diagnostic tool in children with chronic cough. Front Pediatr 2022; 10: 850912.
Marchant JM, Chang AB, Kennedy E, et al. Cough in Children and Adults: Diagnosis, Assessment and Management (CICADA). Summary of an updated position statement on chronic cough in Australia. Med J Aust 2024; 220: 35-45.
Recommendation type: Consensus recommendation
FeNO ≥25 ppb supports the diagnosis of asthma in a child with and signs and symptoms strongly suggesting asthma.
In children and adolescents aged ≥5 years, a FeNO level > 24 ppb has a reported sensitivity of 0.50 and specificity of 0.91 for the diagnosis of asthma.[BTS-NICE-SIGN 2024]
Normal FeNO level does not rule out asthma.
Högman M, Bowerman C, Chavez L, et al; Global Lung Function Initiative FENO Task Force. ERS technical standard: Global Lung Function Initiative reference values for exhaled nitric oxide fraction (FENO50 ). Eur Respir J 2024; 63: 2300370.
The FeNO test is available in accredited respiratory function laboratories. Age restrictions differ between laboratories.
Normal reference ranges for FeNO vary between measuring devices and testing protocols.[Högman 2024]
The test can generally be performed correctly by children 4 years and older.
FeNO is elevated in the presence of active type-2 inflammation of the airway associated with asthma. It is also elevated in some other inflammatory conditions (e.g. allergic rhinitis).
FeNO is suppressed by ICS and systemic corticosteroids.
The FeNO test is more useful for ruling in a diagnosis of asthma than ruling it out. A normal FeNO level does not rule out asthma.
More information on tests of airway inflammation
Arrange either skin-prick testing or serum test for allergen-specific IgE.
Recommendation type: Consensus recommendation
Allergy testing is not recommended as a standalone diagnostic test for asthma, due to its low specificity.[ERS 2021] However, allergy testing at the time of diagnosis is useful to inform management because most children with asthma have allergies, which may affect asthma control.
The presence of allergies in preschool children with asthma-like signs and symptoms is also associated with a higher probability that the child will have asthma at primary school age.[Kothalawala 2020]
The most common aeroallergens causing asthma or allergic rhinitis are dust mites, pollens (most often grass pollen, less often other wind-borne pollens from trees and weeds), animal epithelia, and moulds.[ASCIA 2020]
The history may help identify relevant aeroallergens for testing.
Either skin-prick testing or allergen-specific IgE antibody testing can be used to identify clinically relevant aeroallergens.[ASCIA 2024, ASCIA 2020]
ASCIA. Laboratory investigation for allergic diseases. Australasian Society of Clinical Immunology and Allergy, 2020.
ASCIA. Skin prick testing guide for diagnosis of allergic diseases. Australasian Society of Clinical Immunology and Allergy, 2024.
Gaillard EA, Kuehni CE, Turner S, et al. European Respiratory Society clinical practice guidelines for the diagnosis of asthma in children aged 5-16 years. Eur Respir J 2021; 58: 2004173.
Kothalawala DM, Kadalayil L, Weiss VBN, et al. Prediction models for childhood asthma: A systematic review. Pediatr Allergy Immunol 2020; 31: 616-627.
ASCIA’s Laboratory investigation for allergic diseases (2020)
ASCIA’s Skin prick testing guide for diagnosis of allergic diseases (2025)
Resources
The roles and interpretation of tests for type 2 inflammation in asthma, including fractional exhaled nitric oxide,…

Medication management
How to choose optimal starting treatment for preschool children.

Clinical Topics
Information on risk factors for developing asthma, and on evidence for prevention strategies.