Australian Asthma Handbook
The National Guidelines for Health Professionals
Australian Asthma Handbook
The National Guidelines for Health Professionals
Cite
Table
| Good control | Poor control |
All of these over past 4 weeks: Daytime symptoms ≤2 days per week No limitation of activities No symptoms during night or on waking Reliever use ≤2 days per week* | Any of these over past 4 weeks: Daytime symptoms >2 days per week Any limitation of activities Any symptoms during night or on waking Reliever use >2 days per week* |
Additional information
*Do not include short-acting beta2 agonist (salbutamol or terbutaline) taken prophylactically before exercise. Do not include reliever use for patients using an anti-inflammatory reliever (budesonide-formoterol or beclometasone-formoterol) in an AIR-only or MART regimen.
Table
Factors associated with increased risk of exacerbations Poor asthma symptom control Any asthma exacerbation during the previous 12 months High SABA use (3 or more salbutamol canisters in a year, i.e. average of 1.6 actuations per day/11 actuations per week) Other concurrent chronic lung disease Poor lung function (even if few symptoms) Difficulty perceiving airflow limitation or the severity of exacerbations Eosinophilic airway inflammation (blood eosinophil count ≥300/microlitres despite maintenance treatment with medium-dose ICS) Exposure to cigarette smoke/vapes, smoke from fires Socioeconomic disadvantage Mental illness |
Factors associated with increased risk of life-threatening asthma History of severe exacerbation (intubation/ICU admission due to asthma [ever], 2 or more hospitalisations for asthma in past year, 3 or more ED visits for asthma in the past year, or hospitalisation or ED visit for asthma in the past month) History of sudden-onset acute asthma History of delayed presentation to acute care during moderate–severe exacerbation High SABA use (particularly if 12 or more salbutamol canisters/year, i.e. average 6.6 actuations per day) Comorbid cardiovascular disease Sensitivity and exposure to an unavoidable allergen (e.g. mould) Lack of written asthma action plan Social isolation Socioeconomic disadvantage Mental illness |
Factors associated with thunderstorm asthma Springtime allergic rhinitis or confirmed ryegrass pollen allergy (if exposed to high grass pollen levels during spring and early summer) |
Factors associated with accelerated decline in lung function Chronic hypersecretion of mucus Severe asthma exacerbation when not taking ICS Poor lung function Eosinophilic airway inflammation (blood eosinophil count ≥300/microlitres despite maintenance treatment with medium-dose ICS) Exposure to cigarette smoke Occupational asthma |
Factors associated with adverse effects of treatment Long-term high-dose ICS Frequent use of OCS |
Additional information
ED: emergency department; ICS: inhaled corticosteroids; SABA: short-acting beta2 agonist; OCS: oral corticosteroid
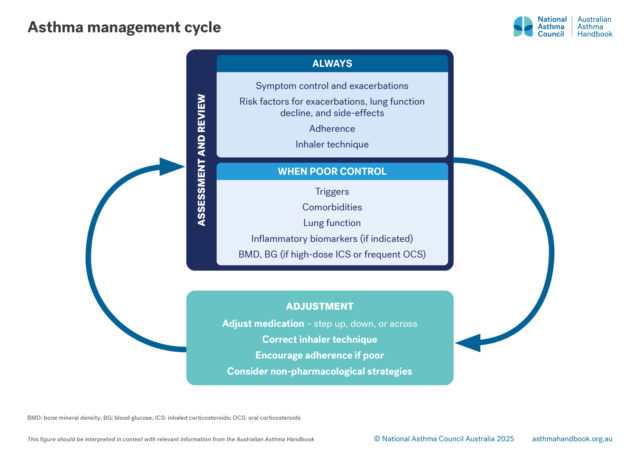
Assess symptom control at asthma-specific visits, and opportunistically at other visits by asking about the previous 4 weeks:
Also ask about asthma since the last visit:
Recommendation type: Consensus recommendation
In addition effects on quality of life, symptom frequency and SABA use are independent predictors of the risk of severe exacerbations.[GINA 2025]
In patients using budesonide-formoterol as needed only without maintenance treatment (recommended level 1 treatment), frequency of reliever use has not been shown to be an independent predictor of risk. However, ongoing need for reliever ≥3 times per week suggests that maintenance treatment with low-dose ICS-formoterol should be added (i.e. switch to MART).
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Good asthma symptom control means few daytime asthma symptoms (≤2 days per week), no limitation of activities due to asthma, no nighttime symptoms or symptoms when waking up, and infrequent reliever use (≤2 days per week, not including doses taken prophylactically before exercise).
Current asthma control is poor if any of these occurred during the past 4 weeks: daytime symptoms >2 days per week, any limitation of activities, any symptoms during night or on waking, reliever use >2 days per week (not including doses taken prophylactically before exercise).
Ask patients about exposure to environmental tobacco smoke as well as smoking.
Consider the possibility of coexisting COPD and asthma in people who smoke or previously smoked.
Recommendation type: Consensus recommendation
Smoking is an independent risk factor for asthma exacerbations and development of persistent airflow limitation.[GINA 2025] Exposure to environmental tobacco smoke is also associated with poor control of asthma.[GINA 2025]
Smoking is the most important risk factor for COPD.[Yang 2024]
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Yang IA, George J, McDonald CF, et al. The COPD-X Plan: Australian and New Zealand Guidelines for the management of chronic obstructive pulmonary disease 2024. Version 2.77, December 2024. Published online 9 April 2025 https://copdx.org.au/copd-x-plan/
Recommendation type: adapted from GINA
Poor control of asthma symptoms is strongly associated with increased risk of severe exacerbation.[GINA 2025]
Patients with a history of severe exacerbations (one or more in the past year, or any asthma exacerbation that required ICU treatment or intubation) have a high risk of further exacerbations.[GINA 2025]
Other independent risk factors for exacerbations include over-use of SABA reliever, inadequate ICS treatment (no ICS, poor adherence to prescribed ICS or incorrect inhaler technique), obesity, chronic rhinosinusitis, GERD, confirmed food allergy, pregnancy, smoking, vaping, allergen exposure (if sensitised), air pollution, major psychological or socioeconomic problems, poor lung function (low FEV1), marked bronchodilator response, and elevated biomarkers of type-2 inflammation (blood eosinophil count, FeNO).[GINA 2025]
Risk factors for developing persistent airflow limitation include preterm birth/low birth weight, chronic mucus hypersecretion, severe exacerbations without ICS treatment, exposure to smoke, airborne irritants or sensitisers, and poor lung function (low FEV1).[GINA 2025]
Also assess risk of systemic adverse events due to frequent courses of systemic corticosteroids, high doses of ICS, or drug-drug interactions with P450 inhibitors.[GINA 2025]
High-dose ICS and incorrect inhaler technique with ICS inhalers are associated with increased risk of local adverse effects such as oral candidiasis and dysphonia.[GINA 2025]
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Obtain spirometry:
Recommendation type: Consensus recommendation
Periodic spirometry is necessary to detect poor lung function, which could deteriorate over time and result in airway remodelling.
Some patients do not experience symptoms when they have poor lung function, so declining lung function may be undetected without spirometry.
More information: Lung function tests
Monitor pre-bronchodilator FEV1.
Withholding of bronchodilators is not necessary before spirometry conducted for monitoring purposes. Withholding is necessary for diagnostic spirometry.
Recommendation type: Consensus recommendation
Spirometry provides more reliable information about lung function than peak expiratory flow measurement.[GINA 2025]
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention, 2025. Available from: www.ginasthma.org
Serial PEF may be required during diagnostic investigation in a patient with suspected work-related asthma.
Adults can perform daily PEF monitoring if they wish. PEF thresholds for action can be incorporated into asthma action plans for adults.
More information: Lung function tests
Recommendation type: Consensus recommendation
Questionnaires validated for use in adults include:
Questionnaires validated for use in adolescents 12–18 years include:
Juniper EF, O'Byrne PM, Guyatt GH, et al. Development and validation of a questionnaire to measure asthma control. Eur Respir J 1999; 14: 902-907.
Juniper EF, Svensson K, Mork AC, et al. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med 2005; 99: 553-558.
Juniper EF, Bousquet J, Abetz L, et al. Identifying 'well-controlled' and 'not well-controlled' asthma using the Asthma Control Questionnaire. Respir Med 2006; 100: 616-621.
Juniper EF, Gruffydd-Jones K, Ward S, et al. Asthma Control Questionnaire in children: validation, measurement properties, interpretation. Eur Respir J 2010; 36: 1410-1416.
Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol 2004; 113: 59-65.
Nguyen JM, Holbrook JT, Wei CY, et al. Validation and psychometric properties of the Asthma Control Questionnaire among children. J Allergy Clin Immunol 2014; 133: 91-97.e91-96.
Schatz M, Sorkness CA, Li JT et al. Asthma Control Test: reliability, validity, and responsiveness in patients not previously followed by asthma specialists. J Allergy Clin Immunol 2006; 117: 549-556.
Schatz M, Kosinski M, Yarlas AS et al. The minimally important difference of the Asthma Control Test. J Allergy Clin Immunol 2009; 124: 719-723.
Thomas M, Kay S, Pike J, et al. The Asthma Control Test (ACT) as a predictor of GINA guideline-defined asthma control: analysis of a multinational cross-sectional survey. Prim Care Respir J 2009; 18: 41-49.
Recommendation type: Consensus recommendation
Approximately 40% of pregnant women with asthma experience worsening asthma symptoms, and at least 20% have an exacerbation that requires medical intervention.[Murphy 2023]
Asthma exacerbations during pregnancy are associated with low birth weight, preterm birth, and small for gestational age status.[Murphy 2023]
Murphy VE, Gibson PG, Schatz M. Managing asthma during pregnancy and the postpartum period. J Allergy Clin Immunol Pract 2023; 11: 3585-3594.
Recommendation type: Consensus recommendation
Long-term high-dose ICS treatment is not recommended.
During an asthma review:

Medication management
How to step up or step down asthma treatment for an individual patient to maintain control and minimise side-effects.

Principles of management
How to choose and use asthma inhalers for adults and adolescents.

Principles of management
How to equip and coach patients to manage their own asthma, including exacerbations.